Jean Carruthers, MD, Alastair Carruthers, MD
TREATMENT OF THE UPPER FACE
Treatment of the upper face with botulinum toxin A (BTX-A) has set a new standard against which all other esthetic procedures are measured. Although the first pub-lished report of BTX application in the face appeared only in 1990, a number of clinicians were already exploring the upper face uses during the late 1980s, enthused by its obvious benefits and safety.1
GLABELLAR RHYTIDES
Four muscles pull the brows together and downward in the inferomedial rotation we call the “frown.” Orbicularis oculi and corrugator superciliaris adduct the brows, and depressor supercilii and procerus move the brows inferi-orly. Individualizing treatment sites and doses to match each subjects’ needs will optimize the clinical benefits. Different injection techniques and doses are described in the literature,1 but recent studies suggest that higher doses may be more effective. In a prospective randomized dose-ranging study of 80 women injected with 10 to 40 U BTX-A, 30 and 40 U produced significantly greater re-sponses with the longest duration on glabellar lines than did 10 or 20 U BTX-A. Both peak responder rates and duration of benefit increased significantly with increasing doses.2,3 At higher doses, many patients experienced clin-ical benefits that lasted 3 to 4 months, but some continued benefit for as long as 6 to 8 months. In an objective pho-tographic analysis of the dose-ranging study, the authors measured changes in eyebrow and eyelid height and found an additional benefit of eyebrow lift at 20 to 40 U peaking at 12 weeks after injection (Fig 1).4 The current recommended doses may not give men as great a benefit as women. In a study comparing the effi-cacy and safety of 4 doses of BTX-A in the treatment of glabellar lines, men were randomly assigned to receive a total of 20, 40, 60, or 80 U in 7 sites.5 Men injected with 80 U achieved a better response rate than those injected with lower doses and experienced no increase in the rate of adverse events. This suggests that male patients are cur-rently considerably underdosed. We find it useful to halve the volume of saline used to reconstitute the vial when treating males. This technique reduces the injected volume while simply doubling the injected dose at each site.
HORIZONTAL FOREHEAD LINES
BTX-A injected across the forehead lessens undesirable horizontal forehead lines for a period of 4 to 6 months.1 We individualize treatment for each patient and keep injection sites well above the brow to avoid brow ptosis or a lack of natural expressiveness. Narrow brows (defined as less than 12 cm between the temporal fusion lines at midbrow level) should receive fewer injections (4 sites compared with 5) and lower doses than patients with broader brows. We previously injected a total of 10 to 20 U in 4 to 5 sites horizontally across the mid-brow, 2 to 3 cm above the eyebrows,1 but—as seen in the glabella—more recent data suggest that higher doses may be more effec-tive. In a prospective, randomized, double-blind, parallel-group, dose-ranging study of 48 weeks duration, 60 women received 16, 32, or 48 U BTX-A in 8 sites in the forehead: 2 in the procerus, 4 in the frontalis, and 2 in the lateral orbicularis oculi (half of the doses were injected into the depressors to protect the brow position).6 BTX-A 48 U led to the greatest improvement and duration of response. Adverse effects, such as headache, eyelid swell-ing, and brow ptosis, were more frequent with the higher doses.
BROW LIFT
Hyperfunction of the brow depressor musculature leads to a lowered brow and angry expression. Medially, the brow depressors include the corrugator supercilii, pro-cerus, and the medial portion of the orbicularis oculi. The only lateral depressor musculature is the lateral portion of the orbicularis oculi. Treating the glabellar lines often also results in brow elevation—the Botox brow lift.1 Huilgol and coworkers report treating the brow depressors alone to elevate the brow while preserving its natural arch.7 One injection of 7 to 10 U in the procerus at the midline followed by 1 injection on each side into the superolateral eyebrow at the temporal fusion line resulted in a modest (mean, 1 mm) brow elevation in 5 of 7 patients. Ahn and coworkers injected 7 to 10 U into the superolateral orbic-ularis oculi at three sites below the lateral third of the brow (but superior and lateral to the orbital rim) and produced average midpupillary elevations of 1 mm and lateral brow elevations of 4.8 mm.8 Huang and coworkers used 10 U in 4 sites along the underside of the lateral half of the brow and 5 U injected into each corrugator muscle just above and medial to the brow.9 Brow height at rest increased by 1.9 mm (on the right side) and 3.1 mm (on the left), while the mean increase in brow height while elevated was 2.1 mm on the right side and 2.9 mm on the left.
The relationship of glabellar treatments and resulting brow height has been further studied in our data from our female glabella dose-ranging study.10 In this study, inject-ing a total of 10 U BTX-A into the glabella produced mild medial brow ptosis, which disappeared after 2 months. Injecting a total dose of 20 to 40 U initially produced only a significant lateral eyebrow elevation, which was fol-lowed by central and medial eyebrow elevation. This ef-fect peaked at 12 weeks after injection but was still present to a significant extent at 16 weeks. We believe this is the first evidence that an effect of BTX-A caused by injection into skeletal muscle has peaked at 12 weeks rather than the usual 4 weeks. Because the primary effect is the lateral brow, which had not been injected—we presume that this brow lift is the result of partial inactivation of the medial fibers of frontalis and not to the action on the brow de-pressors, as previously thought. The subsequent central and medial eyebrow elevation could be due to the reset-ting of the “tone” in the lateral frontalis, causing a gradual brow lift. We believe that further study of this phenome-non will further enhance our ability to give the most excellent esthetic results for our patients.
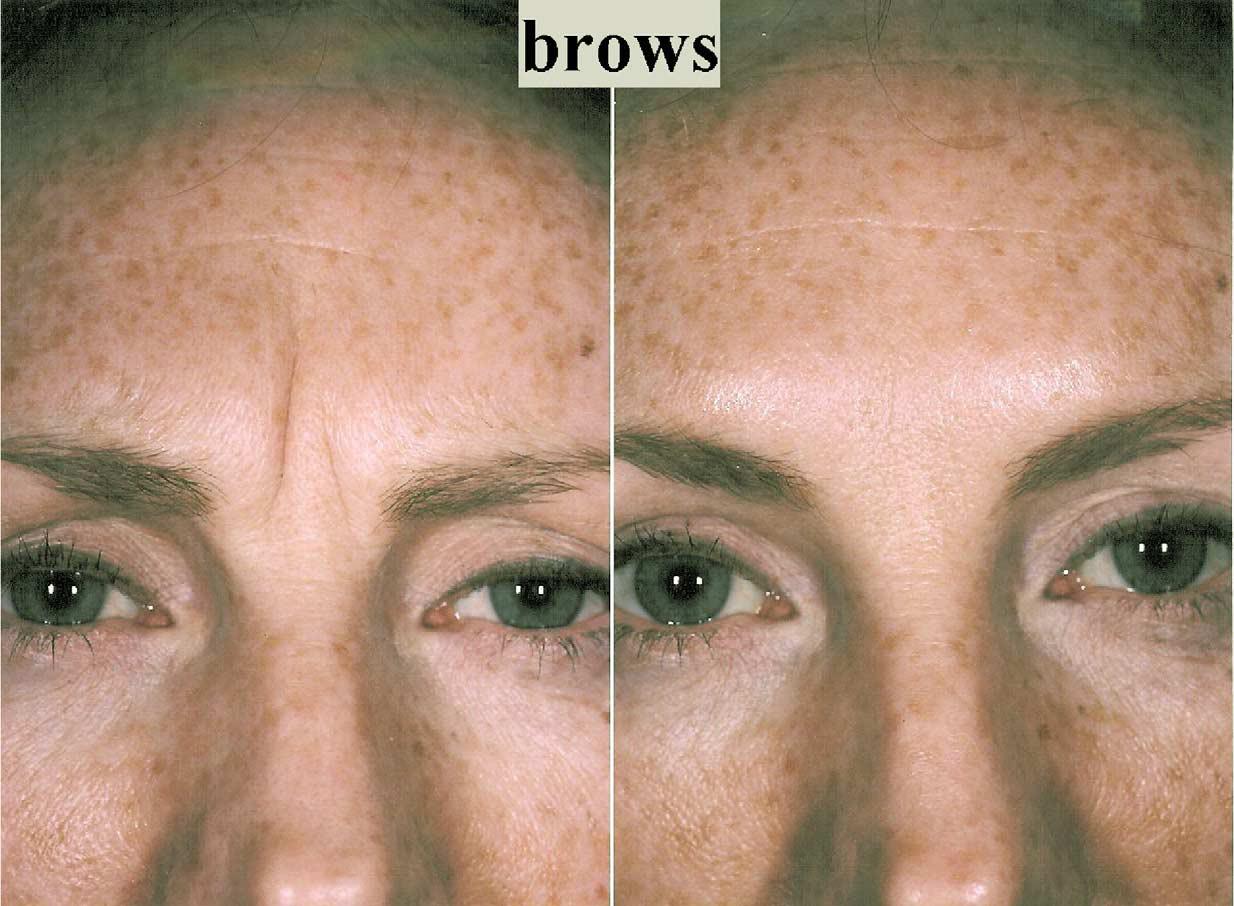
FIGURE 1. It is not just about frown lines but about brow lifting and recontouring. (Color version of figure is available online.)
EYEBROW ASYMMETRY AND SHAPING
Eyebrow asymmetry has many causes, including facial nerve trauma, after surgical brow lifts and other surgically induced facial paralysis. Individuals who are binocular and have ipsilateral eyelid ptosis elevate the brow to clear their visual axis. Asymmetric nonpathologic facial expres-sion as from habitual sleep patterns also are common.11 Injections of BTX-A into the brow depressor muscles on the lower brow side can reset the balance.
MID- AND LOWER FACE AND NECK
BTX-A has to be used with great skill and judgment in the mid- and lower face because of the inherently greater sensitivity of the muscle groups to the treatment in the perioral region. BTX-A treatments, if overdone, can signif-icantly affect function of the all important perioral region. We suggest that previous experience in the indications for the upper face and a complete understanding of the rest-ing and dynamic surface and deep muscular anatomy of the mid and lower face are crucial before injection. Incor-rect injection can result in devastating impairment of func-tion and expression. Electromyographic guidance in some patients is helpful.12
MIDFACE
Crow’s Feet
Contraction of the lateral fibers of orbicularis oculi fold the skin radially from the lateral corner of the eye. Sub-dermally or intradermal BTX-A relaxes the action of the muscle without completely inactivating the orbicularis oc-uli, avoiding reduced ability to fully close the eye. Total doses used range from 4 to 5 U per eye to 5 to 15 U per eye over two or three injection sites. We usually use 12 to 15 U per side, distributed in equal parts over two to four injec-tion sites, and recommend using fewer injection sites as possible to minimize bruising.12 Results generally last from 3 to 6 months, with few adverse effects noted.
Hypertrophic Pretarsal Orbicularis
To electively and nonsurgically widen the palpebral aperture is part of the new esthetic artistry of BTX-A in facial contouring and sculpting. The act of smiling tran-siently diminishes the perceived size of the palpebral ap-erture, notably in Asian patients, who sometimes desire a more round-eyed, “Western” appearance. We inject 2 U into the lower pretarsal orbicularis to relax the palpebral aperture both at rest and while smiling.12 Flynn and co-workers, in a study of 15 women, injected 2 U subder-mally, 3 mm inferior to the lower pretarsal orbicularis. In addition, on one side only, three injections of 4 U were placed 1.5 cm from the lateral canthus, each 1 cm apart.13 Mean palpebral aperture increase in 86% of patients was 1.8 mm at rest and 2.9 mm at full smile, and results were more dramatic in the Asian eye (Fig 2). We suggest the selection of patients who have a good preinjection snap test and who have not had previous lower eyelid ablative resurfacing or infralash blepharoplasties unless they have had a coexisting canthopexy to support the normal posi-tion of the lower eyelid. Goldman reports a case of a 56-year-old man who developed festooning of the in-fraocular area 2 to 3 days following injections of 10 and 2 U BTX-A in the mid-lateral canthal region and 2 to 3 mm below the ciliary margin in the midpupillary line.14

FIGURE 2. BTX-A into the hypertrophic orbicularis in subjects who have normal lower eyelid elasticity (normal snap test) widens the palpebral aperture both at rest and when smiling. (Color version of figure is available online.)
Nasalis “Bunny Lines”
Upper nasalis extends inferolaterally from the bony dor-sum of the nose and its contraction contributes to the development of fanning, radial rhytides called “bunny lines.” Treatment allows the underlying mimetic muscu-lature to relax, softening the lines. The injection site should be superior to the nasofacial groove (containing levator labii superioris and levator labii superioris alaeque nasi), and antero-inferior to the angular vein. We massage gently after injection to help diffuse the toxin. The lower nasalis fibers drape over the lateral nasal ala and can lead to repeated nasal flare, in which nostrils dilate embarrass-ingly and involuntarily in social situations. Injection into the lower nasalis fibers will weaken this involuntary ac-tion.
Perioral Lip Rhytides
Orbicularis oris is the sphincter muscle lying between the skin and mucous membranes of the lips. It encircles the mouth, and blends between the nose and down to the region between the lower lip and chin. Orbicularis causes the lips to close and pucker. Orbicularis oris causes verti-cal perioral rhytides called “smoker’s” or “lipstick” lines. Associated causes include heredity, photodamage, play-ing musical instruments, which require embouchure, and whistling. We inject microdoses (1-2 U BTX-A per lip quadrant) to produce a localized microparesis of the or-bicularis oris. When used with a soft-tissue augmenting agent, the esthetic benefit is enhanced further. We usually increase the BTX-A dilution in this area, injecting a total of 6 U BTX-A (reconstituted in 0.24 mL) in a total of eight injection sites, for 0.75 U in 0.03 mL per injection. We suggest mindful measurement of the injection sites to ensure balance on either side of the columella will help alleviate potential difficulty with postinjection lip propri-oception. Patients who play a wind instrument or a pro-fessional singer/speaker or individuals with unrealistic expectations may not be ideal subjects.
Midfacial Asymmetry
In patients with mid-facial asymmetry caused by inner-vational or muscular causes, BTX-A chemodenervation may be useful. In hemifacial spasm, repeated clonic and tonic facial movements draw the facial midline toward the hyperfunctional side. Relaxation of the hyperfunctional zygomaticus, risorius, and masseter will allow the face to be centered at rest. In contrast, hypofunctional asymme-try, such as that following VII paresis, requires injection in the normofunctional side of 1 to 2 U in the zygomaticus, risorius, and orbicularis, and 5 to 10 U in the masseter For asymmetry of jaw tension, 5 to 15 U BTX-A injected in-traorally into the internal pterygoid can relieve discomfort when chewing and speaking (Fig 3).
LOWER FACE
Depressor Anguli Oris (DAO)
The DAO extends inferiorly from the modiolus to attach into the inferior margin of the mandible on the lateral aspect of the chin. DAO contraction causes a downward turn to the corner of the mouth and a negative, bitter appearance. We initially injected this muscle directly; however, the DAO overlies the depressor labii inferioris, and many patients suffered intolerable, usually asymmet-rical, paresis of depressor labii. We now inject the DAO at the level of the mandible but at its posterior margin, close to the anterior margin of the masseter. Fortunately, the masseter can be easily felt when the teeth are clenched as many patients have difficulty contracting the DAO voluntarily. The aim of treatment is a dose of 3 to 5 U usually significantly weakens this muscle, which is the aim rather than paralysis (Fig 4).

FIGURE 3. BTX-A injected intraorally into the hyperfunctional internal pterygoid will relax muscular tension and alleviate oral and temporomandibular pain. (Color version of figure is available online.)
Melomental Folds
Melomental folds extend from the depressed corner of the mouth to the lateral mentum. They have traditionally been treated with soft-tissue augmentation alone. The combination of soft-tissue augmentation with BTX-A in-jected into the DAO will extend the duration of the aug-mentation.
Mental Crease
The mental crease can be softened by injecting mentalis just anterior to the mentum. We inject 3 to 5 U into mentalis each side of the midline under the point of the mentum. It is important not to inject any higher at the level of the mental crease, since this will also weaken the lower lip depressors and orbicularis oris and cause serious peri-oral weakness, which can persist for 6 months or more. As in the perioral area, weakening, rather than paralysis, is the aim of treatment. Performing injections as described above will relax irregularities caused by trauma or sur-gery.
Peau d’orange Chin
A loss of subcutaneous fat and dermal collagen un-masks the mentalis and depressor labii muscle attach-ments to the skin of the chin. The resulting peau d’orange appearance can be treated with a combination of soft-tissue augmentation and BTX-A injection of the mentalis or BTX-A injections alone depending on the clinical re-quirements.
Mouth “Frown”
Permanent downward angulation of the lateral corners of the mouth is caused by the downward action of the DAO and the upward motion of the mentalis. We have noted that the action of BTX on a single muscle may be associated with a secondary effect on adjacent muscles,producing positive or negative effects. Attempts to weaken the DAO or mentalis alone, while appropriate in some individuals, may be associated with unacceptable side effects in others. We have found that when a lower dose of BTX is injected into both muscles at the same time the weakening effect is both synergistic and safer. Cur-rently, we inject 3 U of BTX-A into each DAO and each mentalis, for a total of 12 U in a female. This produces a subtle effect, which does not interfere with elocution or pursing. This technique, as that for perioral rhytides, should be used only in subjects who have previously positively experienced the effects of BTX in the brow. A hand mirror to demonstrate the aim of treatment is help-ful. Photographs both active and passive before treatment and again at follow up 2 weeks after injection help assess and document the response to treatment, including side effects.
Lower Facial Asymmetry
Decentration of the mouth occurs in patients who have experienced surgical or traumatic cutting of the orbicularis oris or risorius muscle. The unopposed action of the part-ner muscles in the normally innervated side causes the asymmetry. BTX-A injected in the overdynamic risorius, immediately lateral to the lateral corner of the mouth will help to re-center the mouth when the face is in repose. Patients may have congenital or acquired weakness of the DAO, resulting in inability to depress the corner of one side of the mouth; chemodenervation of the contralateral synergistic muscle will restore functional and esthetic symmetry.

FIGURE 4. BTX-A weakening of the depressor anguli oris bilat-erally softens the bitter expression of a persistent mouth frown. (Color version of figure is available online.)
Masseteric Hypertrophy
BTX-A is used for contouring the lateral muscular cheek prominence—a relatively common esthetic procedure among Asians. Ahn and coworkers injected 25 to 30 U BTX-A per side in five to six sites evenly at the prominent portions of the mandibular angle in 45 patients and found a gradual reduction in masseter thickness during the first 3 months after injection (average change in masseter thick-ness, 1.5-2.9 mm, equivalent to 17-19% of the original muscle thickness), as measured by ultrasound and com-puterized tomography.15 The response lasted 6 to 7 months before the muscle thickness retreated to its initial size. At 10 months, 36 patients expressed satisfaction with the results. The local side effects were relatively transient and included mastication difficulty, muscle pain, and ver-bal difficulty during speech.
REFERENCES
- Carruthers A, Carruthers J: Botulinum toxin type A: History and current cosmetic use in the upper face. Semin Cutan Med Surg 20:71-84, 2001
- Carruthers A, Carruthers J: Dose dilution and duration of effect of botulinum toxin type A (BTX-A) for the treatment of glabellar rhyt-ids. Presented at the American Academy of Dermatology 2002 Win-ter Meeting, February 22-27, 2002, New Orleans, LA
- Carruthers A, Carruthers J, Said S: Dose-ranging study of botulinum toxin type A in the treatment of glabellar lines. Presented at the 20th World Congress of Dermatology, July 1-5, 2002, Paris, France
- Carruthers A, Carruthers J: Botulinum toxin type A (BTX-A) in the treatment of glabellar rhytids: An objective analysis of treatment response. Presented at the American Academy of Dermatology 2002 Winter Meeting, February 22-27, 2002, New Orleans, LA
- Carruthers A, Carruthers J: Botulinum toxin type A for treating glabellar lines in men: A dose-ranging study. Presented at the 20th World Congress of Dermatology, July 1-5, 2002, Paris, France
- Carruthers A, Carruthers J, Cohen J: Dose dependence, duration of response and efficacy and safety of botulinum toxin type A for the treatment of horizontal forehead rhytids. Presented at the American Academy of Dermatology 2002 Winter Meeting, February 22-27, 2002, New Orleans, LA
- Huilgol SC, Carruthers A, Carruthers JDA: Raising eyebrows with botulinum toxin. Dermatol Surg 25:373-376, 2000
- Ahn MS, Catten M, Maas CS: Temporal brow lift using botulinum toxin A. Plast Reconstruct Surg 105:1129-1135, 2000
- Huang W, Rogachefsky AS, Foster JA: Brow lift with botulinum toxin. Dermatol Surg 26:55-60, 2000
- Carruthers A, Carruthers J: Glabella BTX-A injection and eyebrow height: A further photographic analysis. Presented at the Annual Meeting of the American Academy of Dermatology, March 21-26, 2003, San Francisco, CA
- Fagien S, Brandt FS: Primary and adjunctive use of botulinum toxin type A (Botox) in facial aesthetic surgery: Beyond the glabella. Clin Plast Surg 28:127-148, 2001
- Carruthers J, Carruthers A: BOTOX use in the mid and lower face and neck. Semin Cutan Med Surg 20:85-92, 2001
- Flynn TC, Carruthers JA, Carruthers JA: Botulinum-A toxin treat-ment of the lower eyelid improves infraorbital rhytides and widens the eye. Dermatol Surg 27:703-708, 2001
- Goldman MP: Festoon formation after infraorbital botulinum A toxin: A case report. Dermatol Surg 29:560-561, 2003
- Park MY, Ahn KY, Jung DS: Botulinum toxin type A treatment for contouring of the lower face. Dermatol Surg 29:477-483, 2003
